
 Because injuries are never planned, be prepared by bookmarking Dr. Steven Chudik's online scheduling tool today!
Because injuries are never planned, be prepared by bookmarking Dr. Steven Chudik's online scheduling tool today!
A midshaft clavicle fracture is a fracture (break) in the middle third or shaft of the clavicle (collarbone). This is the most common location for a clavicle fracture. For significantly displaced midshaft clavicle fractures, open fractures, or fractures associated with other significant nerve, blood vessel, or bone injuries, surgery is recommended. Surgery can stabilize the fracture in proper position to allow healing, movement of the patient and protection for the other associated injuries.
Surgery consists of making a small open incision over the clavicle, repositioning the fracture fragments and holding them in place with plates, screws, wires, sutures or pins. After fracture healing, these fixation devices may be removed, if needed. During surgery, X-ray is used to ensure all fragments are appropriately aligned.
Learn More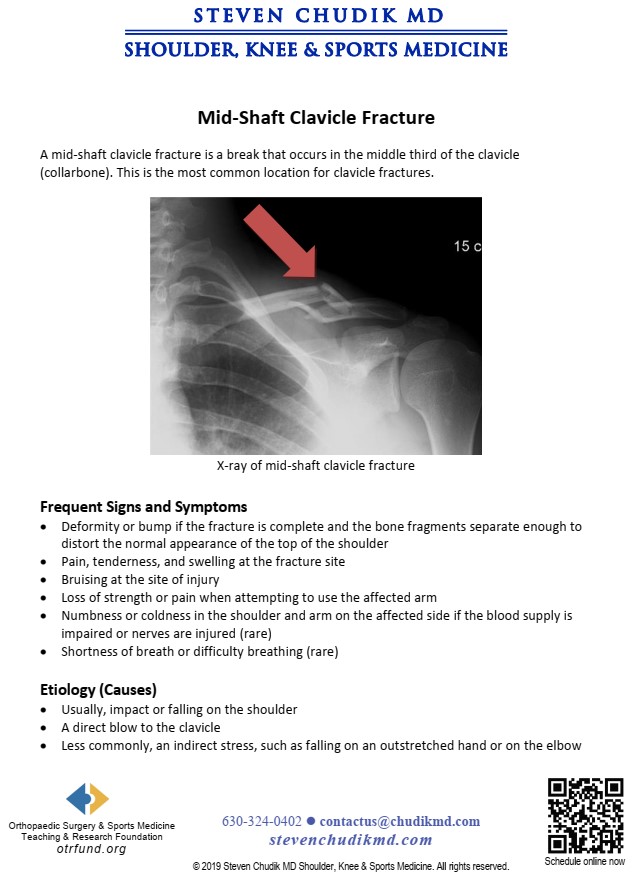
Operative plate fixation of displaced mid-shaft clavicle fractures has been shown to improve the functional outcomes and decrease the likelihood of non-union over non-surgical techniques. The purpose of the study was to biomechanically compare the pull-out strength of two locking bicortical screws versus three non-locking bicortical screws used in plate fixation of midshaft clavicle fractures. We hypothesized there would be no significant difference in pull-out strength between the experimental groups and the load to failure of the two fixation methods would both exceed the reported load to failure in other more physiologic cantilever bending midshaft clavicle fracture-plate biomechanical models.
There was no significant difference in stiffness, cyclic displacement, yield or ultimate load between the constructs. Three non-locking screws demonstrated an average ultimate load of 2496 +/-1102 N, while the two locking screws had an ultimate load of 2715 +/-1150 N. This remained true when examining the data with the removal of outliers, as well as when examining only the desired method of failure (screw pullout).
click below to learn more.
Learn More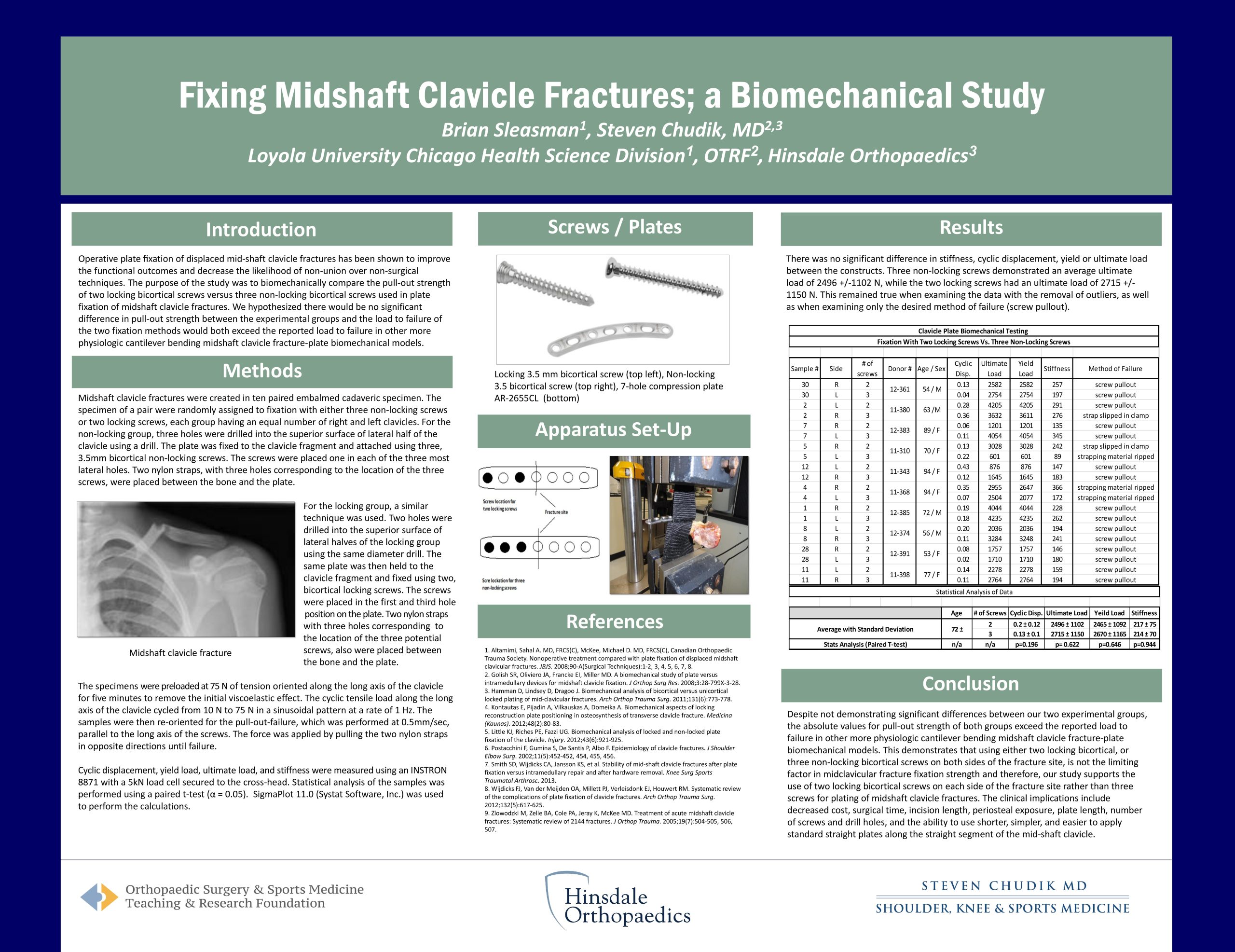
The standard of care for plating displaced midshaft clavicle fractures has been six cortices of purchase on each side of the fracture. The use of locking plates and screws may afford equivalent biomechanical strength with fewer cortices of purchase on each side of the fracture which research studied.
click the link below to learn more
Learn MoreContent provided by Dr. Chudik not to be used for diagnosis and treatment. You can receive a proper evaluation and diagnosis by making an appointment with Dr. Chudik
 Ashford University Senior Student Athlete Award, 2012-13 in recognition of his contributions to the Ashford Athletic Department
Ashford University Senior Student Athlete Award, 2012-13 in recognition of his contributions to the Ashford Athletic Department
Dr Steven Chudik founded OTRF in 2007 to keep people active and healthy through unbiased education and research. Click to learn about OTRF’s free programs, educational opportunities and ways to participate with the nonprofit foundation.
4700 Gilbert Ave, Suite 51
Western Springs, Illinois 60558
Phone: 630-324-0402
Fax: 630-920-2382

© 2026 © 2019 Copyright Steven Chudik MD, All Rights Reserved.



