Shoulder dislocations are injuries where the humeral head (ball) of humerus (upper arm bone) is no longer articulating (in contact) with the glenoid (socket) of the shoulder joint. The most common dislocation is anterior (more than 90 percent), where the humeral head dislocates out in front and below the glenoid socket. Because the shoulder has more motion than any other large joint in the body, it is the most commonly dislocated large joint. There are many structures that work together to provide shoulder stability and include the bone of the humeral head and glenoid, the glenoid labrum (a thickening of soft-tissue surrounding the glenoid socket), the capsule and ligaments which connect the humerus to the glenoid, and the tendons of the rotator cuff muscles which surround the shoulder. Any or all these anatomic structures may be damaged with a shoulder dislocation and may require repair.
Outcomes following traumatic shoulder dislocations depend on the age of the patient and the extent of the pathology. Patients who sustain a shoulder dislocation at an age older than 40 years are less likely to have a repeat dislocation and rarely need surgery to prevent future dislocations. However, patients over the age of forty often suffer a fracture or tear of the rotator cuff with a shoulder dislocation and may require surgery to repair the fracture or rotator cuff. For younger patients, the rate of repeat dislocation and further damage to the shoulder is so high that arthroscopic surgery to repair the torn labrum, ligaments and other structures is often required and recommended after the first dislocation.
Learn More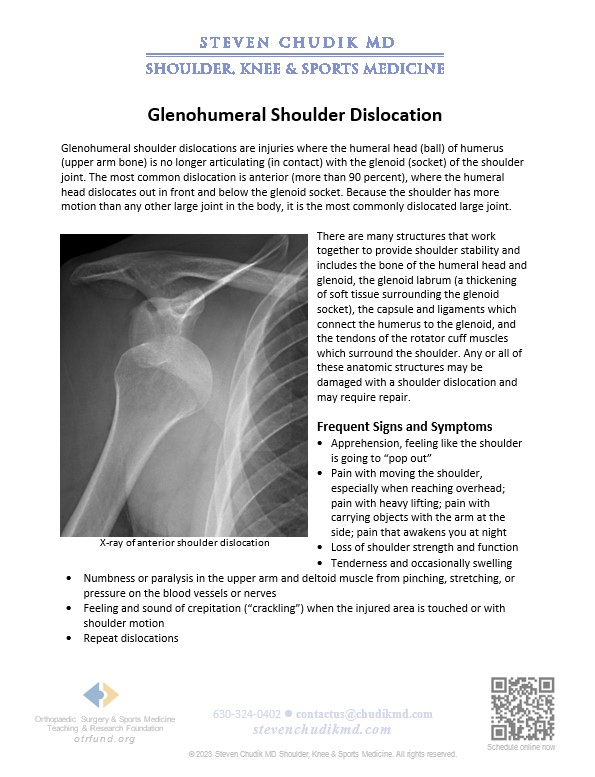
 “Thank you Dr. Chudik for treating Jacob so he could pursue his wrestling goals…The Curby Family.”
“Thank you Dr. Chudik for treating Jacob so he could pursue his wrestling goals…The Curby Family.”
Dr Steven Chudik founded OTRF in 2007 to keep people active and healthy through unbiased education and research. Click to learn about OTRF’s free programs, educational opportunities and ways to participate with the nonprofit foundation.
4700 Gilbert Ave, Suite 51
Western Springs, Illinois 60558
Phone: 630-324-0402
Fax: 630-920-2382

© 2026 © 2019 Copyright Steven Chudik MD, All Rights Reserved.




