
 Because injuries are never planned, be prepared by bookmarking Dr. Steven Chudik's online scheduling tool today!
Because injuries are never planned, be prepared by bookmarking Dr. Steven Chudik's online scheduling tool today!
A midshaft clavicle fracture is a complete or incomplete fracture (break) in the middle third of the clavicle (collarbone) in the shaft. This is the most common location for a clavicle fracture. For significantly displaced midshaft clavicle fractures, open fractures, or fractures associated with other significant nerve, blood vessel, or bone injuries, surgery is recommended. Surgery can stabilize the fracture in proper position to allow healing, movement of the patient, and protection for the other associated injuries.
Surgery consists of making a small open incision over the clavicle, repositioning the fracture fragments, and holding them in place with plates, screws, wires, sutures, or pins. After fracture healing, these fixation devices may be removed if needed. During surgery, X-ray is used to ensure that all fragments are appropriately aligned.
Learn More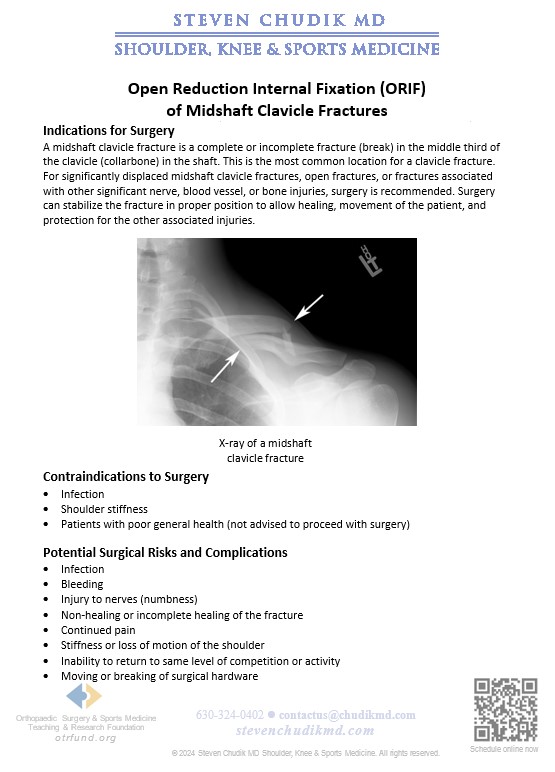
click the link below to learn more
Learn Moreclick the link below to learn more
Learn MoreContent provided by Dr. Chudik not to be used for diagnosis and treatment. You can receive a proper evaluation and diagnosis by making an appointment with Dr. Chudik
 Rotator cuff surgery doesn’t deter golfer or ability to hit a hole-in-one
Rotator cuff surgery doesn’t deter golfer or ability to hit a hole-in-one
Dr Steven Chudik founded OTRF in 2007 to keep people active and healthy through unbiased education and research. Click to learn about OTRF’s free programs, educational opportunities and ways to participate with the nonprofit foundation.
4700 Gilbert Ave, Suite 51
Western Springs, Illinois 60558
Phone: 630-324-0402
Fax: 630-920-2382

© 2026 © 2019 Copyright Steven Chudik MD, All Rights Reserved.



