
Chicago Bulls’ guard Coby White sidelined with torn labrum from neighborhood pick-up game
It was just a friendly neighborhood pick-up game of hoops for Chicago Bulls guard Coby White, or so he thought. According to his recounting of the game, White said he just bumped shoulders doing what he does as a guard. “No big deal and something he’d done before,” he explained.
However, after a couple of days White’s left shoulder still was sore so he flew to Chicago where he had an MRI. The news was not good. White tore the labrum in his left shoulder. When told the news White’s response was, “What’s a labrum?”
Dr. Steven Chudik, orthopaedic surgeon, arthroscopic expert and sports medicine physician with the Shoulder, Knee and Sports Medicine Injury Clinic in Westmont and Western Springs, Ill., said many of his patients through the years have asked the same question.
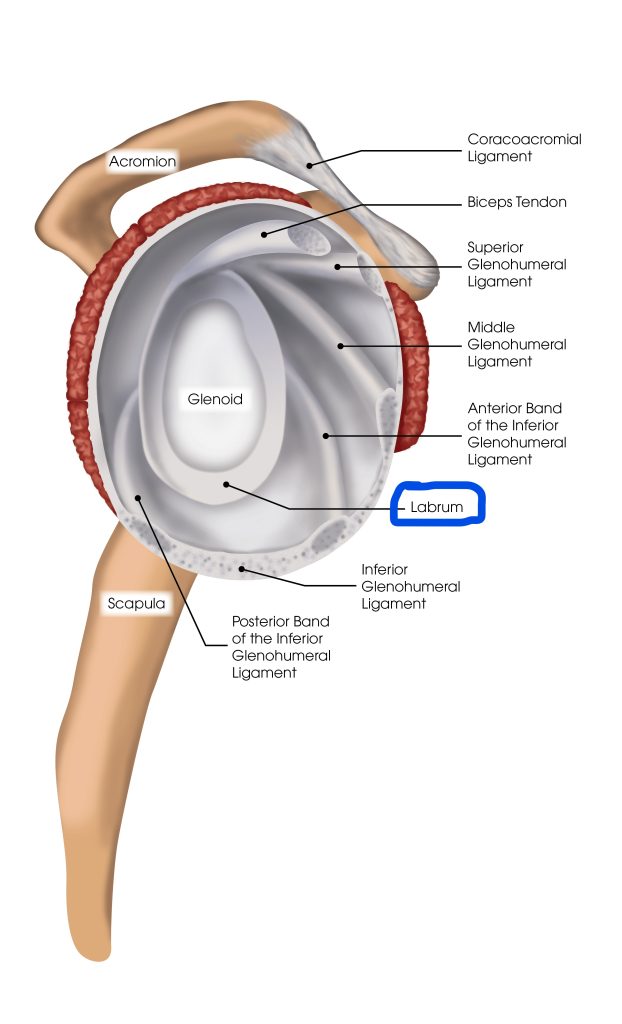
“You don’t hear much about the labrum which is a fibrocartilaginous tissue that circles the peripheral rim of the glenoid (shoulder socket) making it deeper to help hold the humeral head (ball) in place,” Dr. Chudik explained. “It is really the workhorse in the glenoid because it also functions as the attachment site of the shoulder capsule and ligaments that run between the humeral head (ball) and glenoid (socket) of the shoulder to provide stability,” he added.
The long head of the biceps tendon also attaches to the superior (upper) bony glenoid by its attachment through the superior (upper) labrum. Injury to the superior labrum is referred to as a SLAP lesion (tear), which is an acronym for Superior Labrum, Anterior to Posterior (front to back). This tear may take the form of degenerative (wear and tear) fraying, a split in the labrum, or a complete separation of the labrum off the bony glenoid, with or without damage to the biceps tendon attachment. Superior labral separations also result in some lesser amounts of shoulder instability. Superior labral tears are sometimes difficult to see on MRI but are sometimes found during arthroscopic surgery.
Without knowing what type of labral tear White suffered, Dr. Chudik said these are the usual causes:
• Repetitive throwing or overhead hitting motion
• Falling onto the outstretched arm
• Pulling of the arm backwards when overhead
• Sudden force applied to the biceps while contracted
• Direct blow to the shoulder with the arm in a throwing position
• Direct blow to the shoulder that subluxes or dislocates the shoulder
According to Dr. Chudik, labral tears do not heal themselves because of their limited blood supply and the instability (continued motion) of the torn portion; and therefore, they sometimes require surgery. Additionally, physical exam findings are not sufficiently specific to reliably make the diagnosis of a labral tear. MRI and MR arthrograms (MRI following dye injection into the shoulder) are limited and often fail to show clinically significant labral tears. Therefore, after an acute shoulder injury with a history and physical findings consistent with a labral tear or failure of conservative physical therapy, treatment often is needed to confirm an injury.
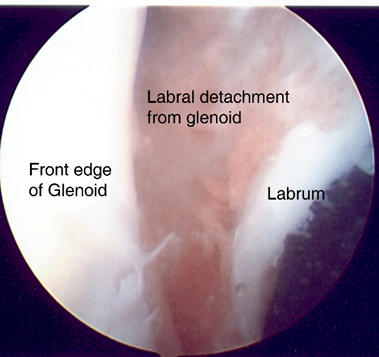
Arthroscopic image of detached (torn) labrum from the glenoid.
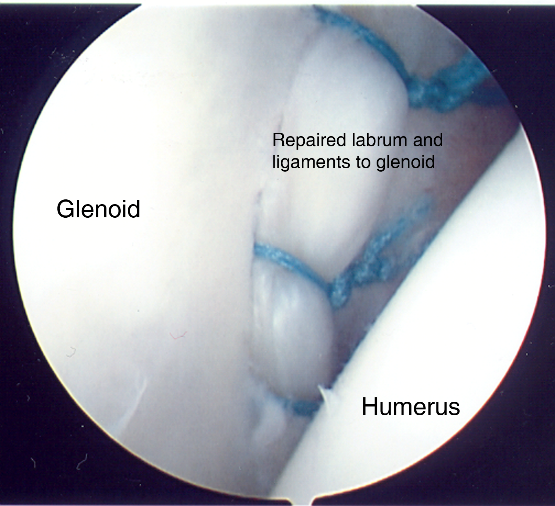
Arthroscopic image of a repaired labrum and ligaments to the glenoid.
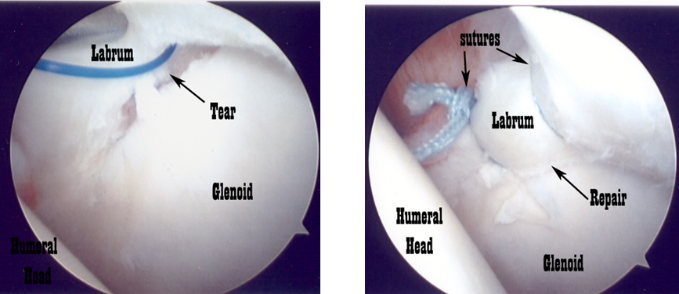
Arthroscopic image of Superior labrum torn from glenoid, left, and repaired back to the glenoid, right.
After four to six weeks of proper shoulder therapy, the majority of milder sprains or strains (that do not need surgery) will improve. A significate labral tear will continue to cause symptoms and produce pain with specific physical exam tests. At this point, arthroscopic surgery would be the recommendation to debride (clean and remove torn labral pieces and torn fragments not detached from the bone) or to repair the separated labrum back to the bone of the glenoid.
Repair (reattachment) of the labrum is performed by placing suture anchors (absorbable) in the bony glenoid, passing the sutures (thread) connected to the anchors through the torn labral portion and tying the sutures securing the labral tissue back in place against the bone. If repair is undertaken, immobilization in a sling is required usually for six weeks to allow the labrum to heal back to the glenoid.
Following surgery and immobilization, physical therapy is recommended for four to six months to regain shoulder motion, strength, and function. According to updates from the Chicago Bulls, White has been rehabilitating his shoulder and will be evaluated at the fourth month mark at which time the team doctors will decide on whether he will be able to come off the bench.
Addressing his progress, White told reporters “I am able to do pretty much everything on a basketball court. I just struggle with left hand, overhead shots like, lay-ups, but I can pretty much do anything else,” he said. “Right now, I’ve just been working on strengthening my shoulder and getting it stronger,” he added.
Dr. Chudik said if White continues to progress with his physical therapy, he should be able to return to play about one month into the season as the team physicians are planning.
If you or someone you know suffered a shoulder injury and needs to be evaluated, contact Dr. Chudik’s office by emailing contactus@chudikmd.com/, calling 630-324-0402, or scheduling online at https://www.stevenchudikmd.com/schedule-online/.






