
 Online appointment scheduling is easy, convenient anytime on any device
Online appointment scheduling is easy, convenient anytime on any device
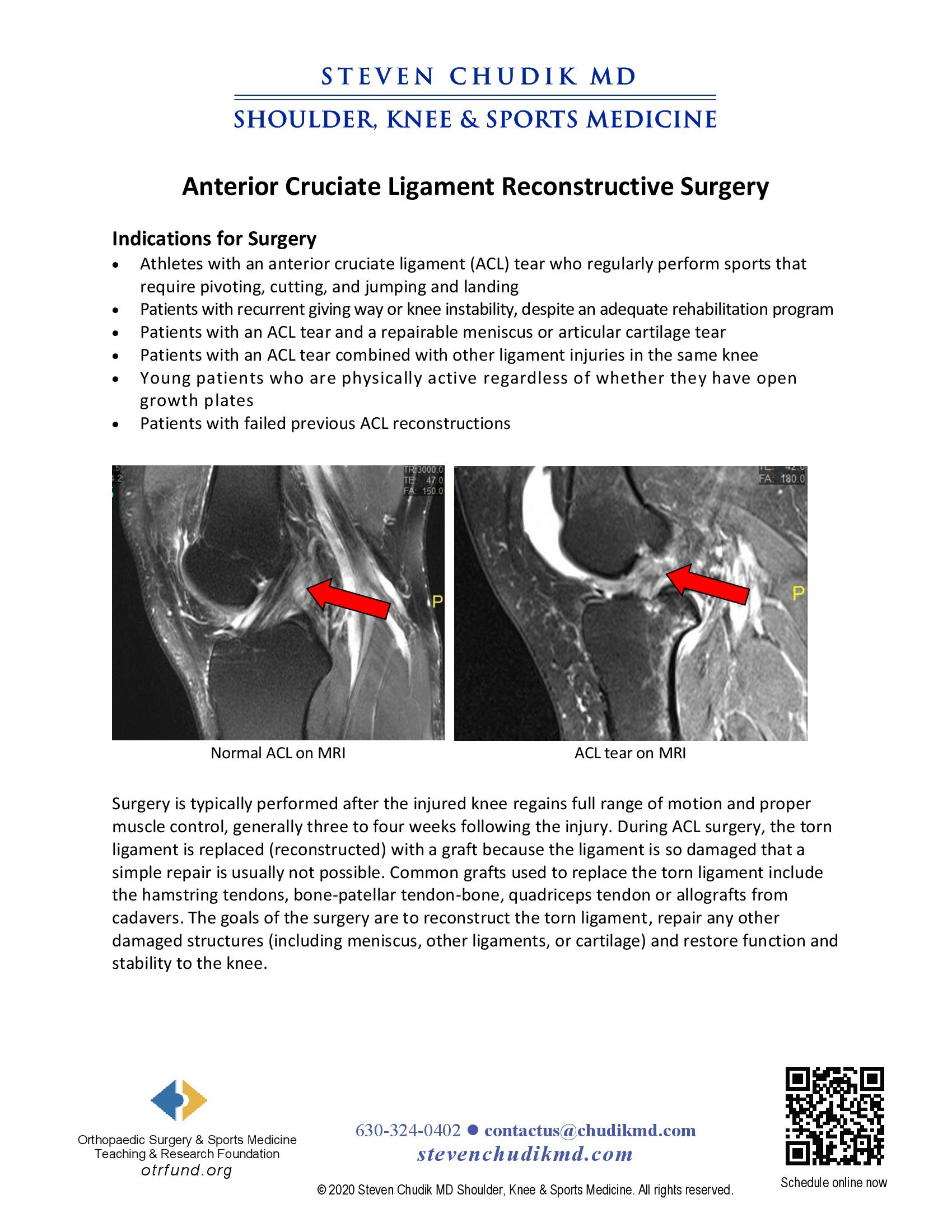
Surgery is typically performed after the injured knee regains full range of motion and proper
muscle control, generally 3 to 4 weeks following the injury. During ACL surgery, the torn
ligament is replaced (reconstructed) with a graft because the ligament is so damaged that a
simple repair is usually not sucessful. Common grafts used to replace the torn ligament include
the hamstring tendons, bone-patellar tendon-bone, quadriceps tendon or allografts from
cadavers. The goals of the surgery are to reconstruct the torn ligament, repair any other
damaged structures (including meniscus, other ligaments, or cartilage) and restore function and
stability to the knee.
click to learn more
Learn More
click to learn more
Learn More
 Competitive running, bicycling back on energetic executive’s schedule between work, volunteering
Competitive running, bicycling back on energetic executive’s schedule between work, volunteering
Dr Steven Chudik founded OTRF in 2007 to keep people active and healthy through unbiased education and research. Click to learn about OTRF’s free programs, educational opportunities and ways to participate with the nonprofit foundation.
4700 Gilbert Ave, Suite 51
Western Springs, Illinois 60558
Phone: 630-324-0402
Fax: 630-920-2382

© 2026 © 2019 Copyright Steven Chudik MD, All Rights Reserved.



