The posterolateral corner (PLC) of the knee consists of many stabilizers that protect the knee against direct varus and rotational forces. The three main stabilizers of the PLC include the lateral (fibular) collateral ligament (LCL), the popliteofibular ligament (PFL), and the popliteus tendon. A few secondary stabilizers that assist are the lateral capsule, hamstrings, and IT Band. A common mechanism of injury to the PLC occurs with a direct blow to the anteromedial knee or forced hyperextension. PLC tears are found commonly with anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL) tears, so this is an important pathology to test following all ligamentous injuries. Posterolateral corner injuries are caused by a force that exceeds the strength of the static stabilizers. This injury may be a result of a direct blow but can also occur with forced hyperextension and non-contact injuries. PLC injuries are often found in conjunction with ACL and PCL tears.
If untreated, a PLC injury will usually result in the knee giving way and recurrent injuries to the knee with sports and often with daily activities. Injuries to the arteries or nerves have a higher risk of poor outcome. Often surgery is required to restore knee stability. Some athletes never return to sports participation after this injury, although the prognosis is much better when there is no injury to the artery and nerves.
Immediate evaluation of knee stability and nerve and vascular function must be performed. Initial treatment consists of medications and ice to relieve pain and reduce the swelling of the knee. Walking with crutches is often recommended. Bracing or casting may also be recommended initially. Rehabilitation of these injuries usually concentrates on reducing knee swelling, regaining knee range of motion, regaining muscle control and strength, functional training, bracing, and education, such as avoiding sports that require pivoting, cutting, changing direction, and jumping and landing. An MRI is likely required prior to surgery to evaluate the extent of damage. Properly timed surgical repair or reconstruction (replacement) of one or more structures, in the hands of an experienced orthopedic surgeon, has the best chance for an optimal result. Some athletes never return to sports, although often this depends on the associated injuries and the demands of the sport.
Learn More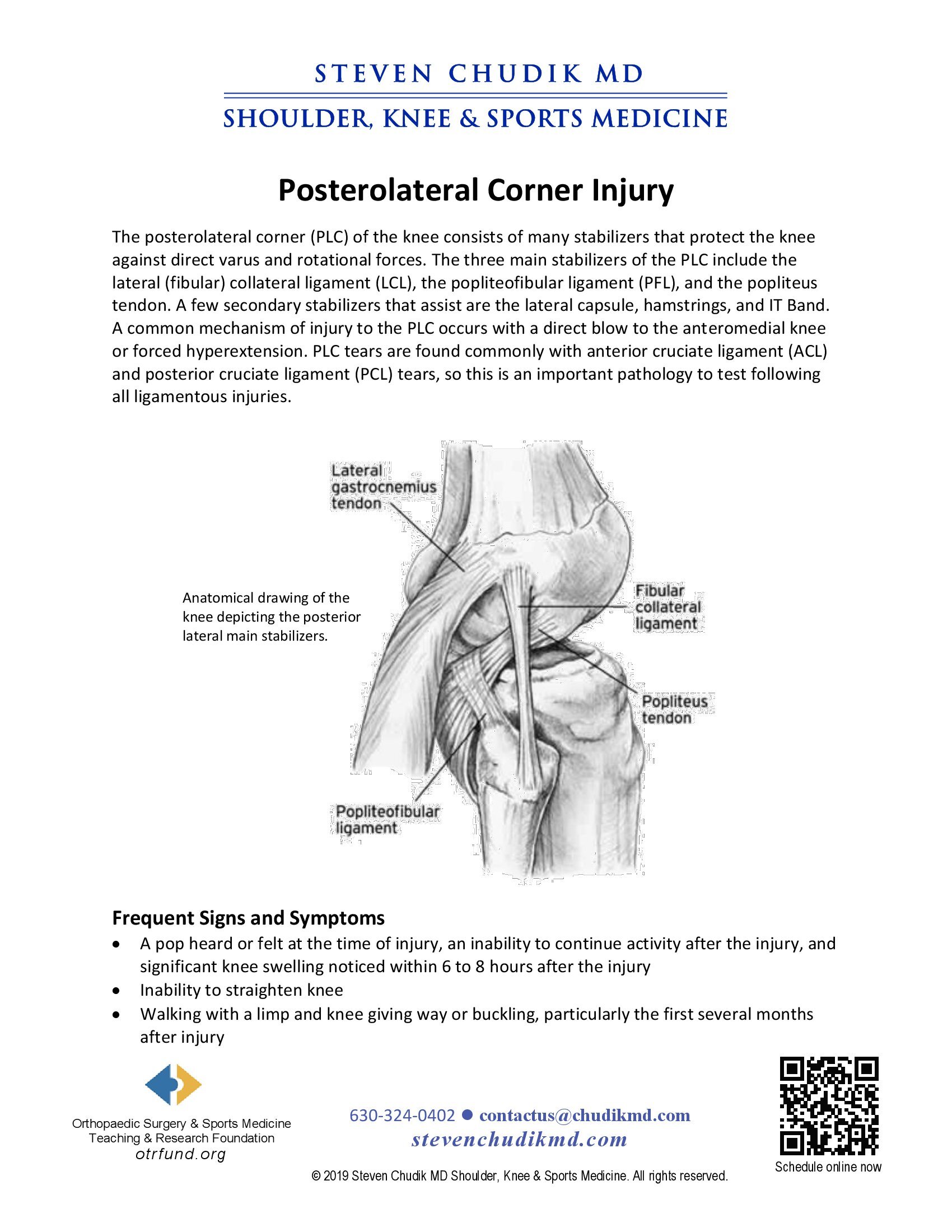
 Knee replacements, customized care plan have Irwin cheering again from the bleachers and soccer fields
Knee replacements, customized care plan have Irwin cheering again from the bleachers and soccer fields
Dr Steven Chudik founded OTRF in 2007 to keep people active and healthy through unbiased education and research. Click to learn about OTRF’s free programs, educational opportunities and ways to participate with the nonprofit foundation.
4700 Gilbert Ave, Suite 51
Western Springs, Illinois 60558
Phone: 630-324-0402
Fax: 630-920-2382

© 2026 © 2019 Copyright Steven Chudik MD, All Rights Reserved.




